Klebsiella pneumoniae
Klebsiella pneumoniae is the most clinically relevant species within the Klebsiella genus, a group of Gram-negative bacteria belonging to the Enterobacteriaceae family. It plays a significant role as an opportunistic pathogen, mainly associated with healthcare-associated infections. It is a common cause of nosocomial infections in intensive care unit (ICU) patients, neonates, individuals with chronic obstructive pulmonary disease (COPD), diabetes mellitus, or alcoholism.
Clinical features: K. pneumoniae is responsible for urinary tract infections, pneumonia, sepsis, surgical wound infections, and soft tissue infections. It accounts for approximately 1% of all bacterial pneumonias and may cause massive hemorrhagic consolidation of the lung, often progressing to lung abscesses or empyema. In immunocompromised or debilitated patients, localized infections can lead to bacteremia with a high risk of mortality.
It is also involved in post-surgical infections, particularly following thoracotomy for coronary artery bypass grafting. In such cases, treatment includes a combination of imipenem (1 g IV every 6 hours for 21 days) and ciprofloxacin (400 mg IV every 12 hours for 21 days), together with aggressive wound care and hydrogel application (Intrasite Gel), with secondary-intention wound closure being the norm. Hypervirulent strains (hvKp) have emerged and are associated with severe invasive disease (e.g., liver abscesses) even in healthy individuals.
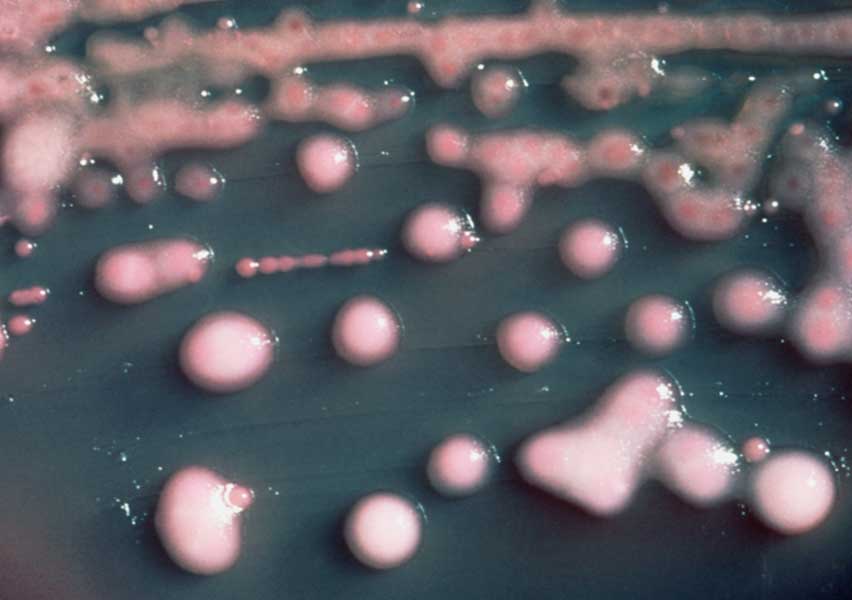
Diagnosis: Initial diagnosis is clinical, especially in pneumonia, where chest radiographs often show lobar consolidation and necrotizing features. Definitive diagnosis is achieved by culture of clinical specimens—such as respiratory secretions, urine, blood, or pus from infected wounds. Colonies typically appear mucoid due to their polysaccharide capsule. Antibiotic susceptibility testing is crucial, as multidrug-resistant (MDR) strains, including those producing extended-spectrum beta-lactamases (ESBLs) or carbapenemases (e.g., KPC), are increasingly prevalent.
Treatment: Management depends on antibiotic susceptibility. Sensitive strains can be treated with third-generation cephalosporins or fluoroquinolones. ESBL-producing strains usually require carbapenems (e.g., imipenem or meropenem). Carbapenemase-producing strains may require combination therapies involving colistin, tigecycline, fosfomycin, or ceftazidime-avibactam. Management also includes the removal of contaminated devices and drainage of abscesses when needed. The rising antibiotic resistance of K. pneumoniae represents a serious global health concern, necessitating strict infection control measures and continuous surveillance.