


Aspergillus fumigatus: Characteristics, Clinical Relevance, Diagnosis and Treatment
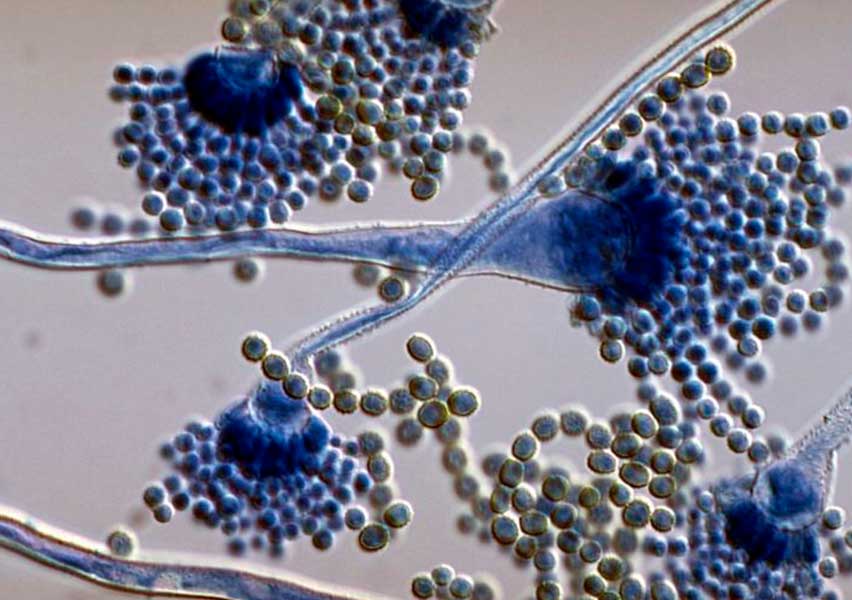
Aspergillus fumigatus is a ubiquitous hyaline filamentous fungus, characterized by short conidiophores and sub-spherical conidia (2–3 µm in diameter). This mold is found worldwide and can grow on almost any substrate, including soil, water, plants, organic debris, and food. Inhalation of its airborne conidia may lead to a broad spectrum of diseases, ranging from allergic asthma in atopic individuals to severe invasive aspergillosis in immunocompromised patients.
Clinical Characteristics
The genus Aspergillus includes more than 180 species of septate hyaline molds that typically branch dichotomously at acute angles. They reproduce mainly asexually through conidiophores, producing large numbers of conidia. The most clinically important species are A. fumigatus, A. flavus, A. niger, and A. terreus. Among them, A. fumigatus is the most pathogenic and the primary cause of invasive aspergillosis.
These fungi thrive in warm and humid environments and are commonly detected in soil, air, water, dust, and food. Despite frequent exposure, immunocompetent individuals rarely develop invasive disease thanks to mucociliary clearance and alveolar macrophages. In contrast, immunocompromised patients—such as those with severe neutropenia, transplant recipients, individuals receiving corticosteroids or immunosuppressive therapy—are at high risk of developing invasive aspergillosis. Less commonly, the disease appears in patients with chronic granulomatous disease, advanced HIV/AIDS, or hereditary immunodeficiency syndromes.
Corticosteroids are a well-known risk factor, as they impair oxidative killing by pulmonary macrophages, increase fungal growth rate by 35%, and enhance cell synthesis by up to 150%.
Diagnosis of Aspergillus fumigatus Infections
Diagnosis can be achieved through several methods, including:
Direct microscopic examination of clinical samples
Fungal culture
Skin testing and serological assays
PCR and molecular diagnostic tools
Imaging techniques such as chest X-ray and CT scan
Treatment of Invasive Aspergillosis
Voriconazole is currently the first-line treatment for invasive aspergillosis. Alternative antifungal therapies include lipid formulations of amphotericin B, itraconazole, caspofungin, micafungin, and posaconazole. Whenever possible, immunosuppressive therapy should be reduced or discontinued to improve clinical outcomes.